
Malaria is a life-threatening disease transmitted by female anopheles mosquitoes. Sub-Saharan Africa carries the major burden of this disease. Malaria has the highest burden of disease in Nigeria – with an estimated 300,000 children dying of malaria each year. Eight-eight percent of the malaria cases in the world are in sub-Saharan Africa. Ninety percent of the malaria deaths are also in Africa.
Here's 7 amazing things you probably didn't know about malaria.
Here's 7 amazing things you probably didn't know about malaria.
1. The name malaria was derived from Mal aria ('bad air')
Malaria also known as Roman fever, ague, marsh fever and periodic fever, was believed by the Romans to be caused by swamp fumes, although indeed it was the swamp-dwelling mosquitoes.Malaria has shaped the course of history for millennial. It has always been part of the ups and downs of nations; of wars and of upheavals.
It is believed that Alexander the Great was killed by malaria at the height of his power. He had set out to subjugate the earth but just as he was to depart with his army in early June 323 B.C., he contracted a fever and the voyage was postponed. At first the thirty-three-year-old general regarded his illness as nothing more than a temporary setback. But Alexander continued to deteriorate until he lapsed into a deep coma and died.
Malaria was the most important health hazard encountered by U.S. troops in the South Pacific during World War II, where about 500,000 men were infected. According to Joseph Patrick Byrne, "Sixty thousand American soldiers died of malaria during the African and South Pacific campaigns."[1]
2. Malaria is caused by the Plasmodium parasite in Anopheles mosquitoes.
Mosquitoes are considered one of the most dangerous creatures on the planet because of their ability to spread deadly diseases. Diseases transmitted by mosquitoes include: dengue, West Nile virus, chikungunya, yellow fever, filariasis, tularemia, dirofilariasis, encephalitis, Ross River fever, Barmah Forest fever and Zika fever, as well as newly detected Keystone virus.
The genus Plasmodium includes over 170 different species that infect mammals, reptiles, birds, and amphibians. However, Human malaria is caused by five different species of Plasmodium: P. falciparum, P. malariae, P. ovale, P. vivax and P. knowlesi.
P. falciparum accounted for 99.7% of estimated malaria cases in the WHO African Region in 2017, as well as in the majority of cases in the WHO regions of South-East Asia, Eastern Mediterranean and the Western Pacific.
P. vivax is the predominant parasite in the WHO Region of the Americas, representing 74.1% of malaria cases [2]
3. The Global Fund provides nearly 60 percent of all international financing for malaria
Top malaria research funders include the US National Institutes of Health, the European Commission, the Wellcome Trust, and the Bill & Melinda Gates Foundation, collectively investing about $37·1 billion into global health research each year, and malaria is a research priority or part of a wider focus for these organisations.4. Government Reservation Area (GRA) were established to prevent malaria
In Nigeria, before independence, the colonialists established Government Reservation Areas (GRA) in an attempt to build their homes far away from the natives, as it was found that the travelling/flying distance of these mosquitoes from the breeding grounds was a limiting factor in spreading the parasites. [3]5. RTS,S/AS01 (RTS,S) the first approved malaria vaccine in stage IV Clinical Trial
Mosquirix Malaria vaccine is a first generation vaccine known as RTS,S/AS01 (RTS,S) acts against Plasmodium falciparum. It requires four injections, and has a relatively low efficacy. The vaccine provides partial protection against malaria among young African children, the population most affected by the disease. Rigorous clinical testing in 7 African countries has shown its potential to boost malaria prevention and save lives.
Another promising malaria vaccine is the irradiated whole sporozoite PfSPZ Vaccine made by Sanaria. Recent trials have shown that it’s safe and well tolerated and had promising protection against malaria when administered intravenously.
However, key limitations for the success of malaria vaccines is the difficulty in maintaining durable protection after immunisation, which in part has been ascribed to poorly immunogenic antigens as well as to the effect of malaria itself in suppressing host responses[4]
6. Quinine the first effective antimalarial was discovers in the 16th century
In the early 15th century, the Bark of the cinchona tree (Fever Tree) was used by the Quecha Indians of Peru to reduce the shaking effects caused by severe chills. It would be nearly 200 years after, before the active compound, quinine and other alkaloids, of cinchona bark were isolated.Below is the current WHO recommendation for management of malaria[5]
Diagnosis of malaria
All cases of suspected malaria should have a parasitological test (microscopy or Rapid diagnostic test (RDT)) to confirm the diagnosis.
Treating uncomplicated P. falciparum malaria
o Treat children and adults with uncomplicated P. falciparum malaria (except pregnant women in their first trimester) with artemisinin-based combination therapies (ACT)
o Duration of ACT treatment: 3 days’ treatment
Treating uncomplicated P. falciparum malaria in special risk groups
o First trimester of pregnancy: 7 days of quinine + clindamycin
Treating severe malaria
o Treat adults and children with severe malaria (including infants, pregnant women in all trimesters and lactating women) with intravenous or intramuscular artesunate for at least 24hr and until they can tolerate oral medication. Complete treatment with 3 days of ACT
o If artesunate is not available, use artemether in preference to quinine for treating children and adults with severe malaria.
7. Chloroquine resistance in P. falciparum was first observed in Thailand in 1957
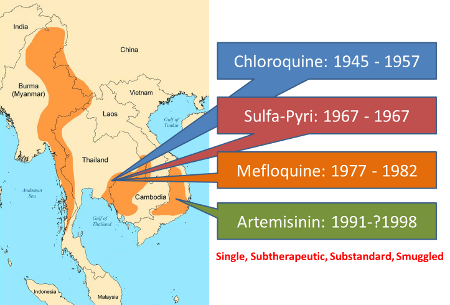

In 1955, WHO launched the most ambitious Global Malaria Eradication Programme; DDT was sprayed everywhere across Asia and South America and chloroquine was used extensively to treat malaria. In many areas, particularly in SE Asia and S America, mass administration of chloroquine was also started as a preventive measure and it was administered to even those who did not have malaria. As a result of this wide spread use, very soon chloroquine resistance in P. falciparum was observed; first in Thailand in 1957 and on the Colombia-Venezuela border in 1959.[6]
Evidence of resistance to artemisinin-based combination therapy (ACT) is being reported. ACTs are taking longer time to clear parasite load from patients. There is therefore a need to develop next generation drugs to address the rising incidence of drug resistance.






No comments:
Post a Comment